PLAIN RADIOGRAPHIC DIAGNOSIS OF CONGENITAL HEART DISEASE |
Contents | Previous Condition | Next Condition
The first reported case of dextrocardia was by Fabricius in 1606. The incidence of situs inversus is reported to be 1:2500 to 1:20,000. Dextrocardia with situs solitus is less common. There is a higher incidence of congenital heart anomalies in isolated destrocardia.
In one autopsy series by Van Praagh there were 239 cases of dextrocardia: 126 had situs solitus, 36 situs inversus, and 77 situs ambiguus.
Embryology: The primitive cardiac loop normally bends to the right at the eight somite stage (day 22-23 gestation). Over the subsequent 10-12 days, during cardiac septation, tha apex of the heart gradually migrates from the right side of the thorax to lie in the left chest pointing leftward. Lack of migration results in dextrocardia.
Dextroversion, dextrorotation, and pivotal dextrocardia are synonymous with dextrocardia with situs solitus. Dextroposition means the heart has been shifted rightward by external causes. Mixed dextrocardia indicates dextrocardia with atrioventricular discordance. Mirror image dextrocardia refers to patients with situs inversus.
The incidence of congenital heart disease varies from 10% in situs inversus to 90% in situs solitus. Cases associated with congenital diaphragmatic hernia have a higher incidence of associated cardiac malformations.
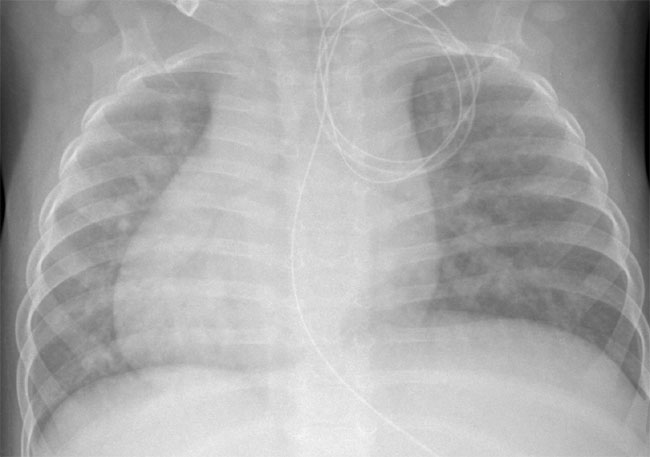
CXR: The situs of the abdominal organs will give an indication of the likelihood of congenital heart defects. The liver and gastric bubble should be sought on a plain abdominal film.
ECG: A p vector directed leftward and inferiorly indicates probable atrial situs solitus; a rightward p wave axis suggests situs inversus.
| Associated defects: | Dextrocardia |
|
| Lesion | Situs Solitus | Situs Inversus |
| 1. L-looped ventricles | 50% | 25% |
| 2. Single ventricle | 25% | |
| 3. VSD | 60% | 60% |
| 4. Corrected Transposition | 50% | 20% |
| 5. TGA | 10% | 30% |
| 6. DORV | 10% | 30% |
| 7. PS/Pulmonary atresia | 60% | 50% |
| 8. Right aortic arch | 5% | 80% |
Scimitar syndrome must always be ruled out in the presence of dextrocardia and situs solitus of the atria and viscera. This is characterized by hypoplasia of the right lung, and anomalous pulmonary venous connection from the right lung to the inferior vena cava. Of note is the discrepancy in frequency of associated defects between the two forms of situs. Patients with situs inversus usually have a right sided aortic arch.
Dextrocardia with situs inversus is also associated with lung anomalies including Karthagener’s syndrome (15-20% of patients). This is characterized by bronchiectasis, chronic sinusitis, nasal polyposis and infertility secondary to immotile spermatozoa. This syndrome is attributed to immotile cilia secondary to a defect in the dynein arm.