PLAIN RADIOGRAPHIC
DIAGNOSIS OF CONGENITAL HEART DISEASE |
Contents | Previous
Condition | Next Condition
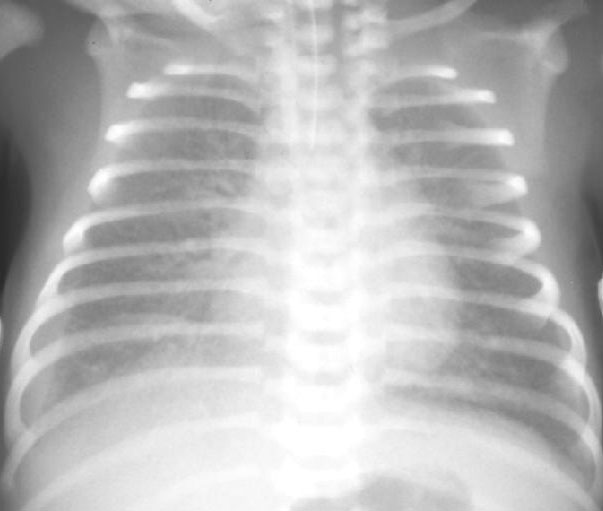
2e-1. Total anomalous pulmonary venous connection (Supracardiac). (Legend.)
A. There is cardiomegaly with increased pulmonary arterial markings. There is dilation
of both the left and right innominate veins and the right superior vena cava producing the
classical "snowman" or "figure of 8" appearance. The superior
mediastinum is enlarged secondary to dilation of the right vena cava, innominate vein and
ascending vertical vein.

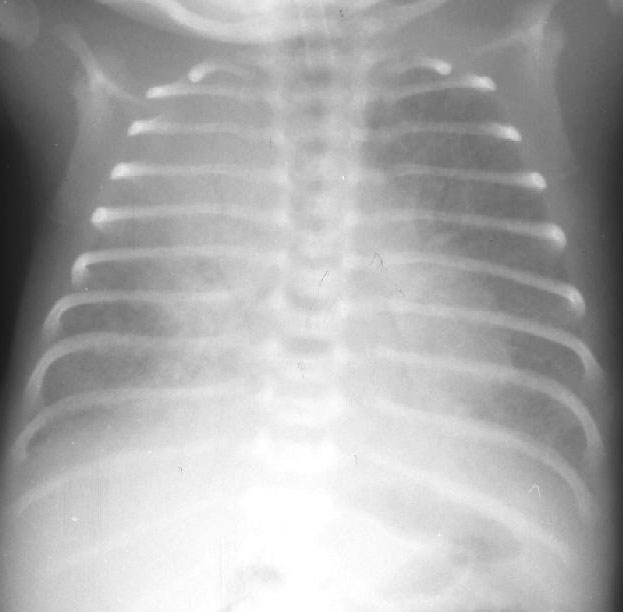
2e-2. TAPVC (Supracardiac).
A. PA chest radiograph shows mild cardiomegaly, increased pulmonary vascular markings
and "snowman" appearance of supracardiac anomalous drainage.

2e-3. Total anomalous pulmonary venous connection (infradiaphragmatic-obstructed).
A. PA chest radiograph demonstrates increased pulmonary venous pattern with a normal
sized heart. There is a right sided pleural effusion. The endotracheal tube is just above
the level of the carina.
2e-4. TAPVC (infradiaphragmatic-obstructed).
A. The heart is normal sized with increased pulmonary venous pattern preferentially in
the right upper lobe.
Total anomalous pulmonary venous connection (TAPVC)
Total anomalous pulmonary venous connection is preferable to anomalous venous return as
one may have anomalous drainage in the absence of anomalous connection. Winslow reported
the first documented case of PAPVC in 1739 in a patient with a right upper pulmonary vein
draining to the superior vena cava.
Anomalous pulmonary venous connection is classified as either partial or total. In
TAPVC all the pulmonary veins drain into the right atrium either directly or via a venous
channel. In all cases there is an ASD or patent foramen ovale which allows right to left
atrial shunting in order to maintain survival. Approximately 1/3 of patients with TAPVC
have other associated cardiac lesions including single ventricle, atrioventricular septal
defect, transposition of the great arteries, hypoplastic left heart syndrome or patent
ductus arteriosus. Many of these patients have heterotaxy syndrome with atrio-visceral
situs abnormalities and polysplenia/asplenia (Ivemark syndrome).
Incidence: TAPVC accounts for less than 1% of all cardiac defects. There is a 3:1 male
preponderance in infants with infradiaphragmatic TAPVC.
Classification:
- Type 1: Supracardiac connection (55%); connection to the left innominate vein is the
commonest accounting for some 44% of all TAPVC. Typically two anomalous veins from each
lung converge directly behind the left atrium and form a common anomalous vertical vein,
which passes anterior to the left pulmonary artery and the left main bronchus. Obstruction
in this lesion is uncommon. However extrinsic compression may occur in cases where the
anomalous vein courses between the left pulmonary artery anteriorly and the left main
bronchus posteriorly. Anomalous connection to the right superior vena cava is much less
frequent but often associated with heterotaxy syndrome/ multiple complex congenital
lesions.
- Type 2: Cardiac connecion (30%); the pulmonary veins connect at the level of the
coronary sinus or in the posterior right atrium near the mid-atrial septum. The anomalous
veins may connect via a short channel or multiple openings to the right atrium. The
coronary sinus ostium is markedly enlarged although normal in position. One paper reported
a 22% incidence of obstruction in this lesion.
- Type 3: Infracardiac connection (13%); this lesion is virtually always accompanied by
some degree of obstructed venous return. The pulmonary veins from both sides converge
behind the left atrium and form a common vertical descending vein, which courses anterior
to the esophagus and traverses the diaphragm at the esophageal hiatus. This vertical vein
may join the portal venous system (80-90% cases) either at the splenic or splenic-superior
mesenteric venous confluence. Occasionally the vertical vein may connect directly to the
ductus venosus or even the hepatic or inferior vena cava. Obstruction to venous drainage
may obviously occur at any point along the abberant path including the esophageal hiatus,
the portal venous system or the ductus venosus (discrete). Obstruction may also occur at
the level of the hepatic sinusoids (diffuse obstruction). Presentation is generally in the
early newborn period.
- Type 4: Mixed pattern (2%); the commonest pattern of mixed obstruction is drainage of a
vertical vein to the left innominate vein and drainage of the right lung either via the
right atrium or the coronary sinus. This pattern of anomalous venous connection is
generally associated with other major cadiac lesions.