Patient #19, a 42 year old white female, presented to the Department of Neurology with a two day history of double vision. She was in her normal state of good health until two weeks prior. At that time, she developed a cough with productive sputum, fever, decreased energy, and headache. She saw her family doctor who prescribed erythromycin, benedryl, and cough syrup. During her convalescence, she slept, took her medications, and ate canned goods. She did improve and returned to work, however a dry, hacking cough persisted. Subsequently, she developed double vision in all directions. She saw an ophthalmologist who felt she had a viral infection and recommended an eye patch. The following morning, the patient awoke with slurred speech, dizziness, headache, extreme fatigue, double vision, difficulty swallowing, and tingling in her hands. She then presented to the Emergency Room.
Past Medical History: No medical problems, no previous similar symptoms, and no recent vaccinations.
Past Surgical History: Tonsillectomy in 1958, removal of heel spurs bilaterally 1982.
Allergies: Penicillin.
Medications: A ten day course of erythromycin with benedryl and cough syrup as needed.
Family History: Mother is 66 years old and has no medical problems. Her father died at the age of 66 from lung cancer and asbestosis. She has two healthy brothers, ages 45 and 39 and no sisters or children.
Social History: She spent her early life in New Jersey and the past 18 years in Houston. She is divorced, lives alone except for a small dog. She does not smoke and is a social drinker. She denies illicit drug use. She is employed as a stage technician. Denies travel outside of the country.
Review of Systems: She complained of some nausea without vomiting, dyspnea, dysphagia although no choking, a 5-10 pound weight loss, diffuse headache, dry mouth, dizziness described as light-headedness, tingling in her hands and a feeling that her teeth were numb. She denied sore throat, abdominal pain, dysuria, diarrhea, or constipation.
General: Overweight white female, uncomfortable but not in distress.
Vital Signs: Temperature 98; Respiration 16; Blood Pressure 114/60 and Pulse 86 while lying; Blood Pressure 110/60 and Pulse 94 while standing; Vital Capacity 1.5 liters.
HEENT: NC/AT, sclera clear, OP clear, TMs clear.
Neck: Supple with some mild pain on neck flexion, no bruits, thyroid not enlarged, no lymphadenopathy.
Chest: Poor inspiratory effort; however no wheezes, rales, nor rhonchi heard.
Cardiovascular: RRR with no murmurs, rubs, or gallops.
Abdomen: Soft, positive bowel sounds, nontender, nondistended, no organomegaly.
Extremities: Pulses intact in all extremities, no edema.
Skin: No rashes present, no ticks noted.
Mental Status: Awake, alert, oriented and cooperative.
Cranial Nerves:
Cranial Nerves | Findings |
|---|---|
| I | Not tested. |
| II | Pupils 6 mm bilaterally, sluggishly reactive, visual acuity 20/20 in both eyes, no field cuts, fundi revealed sharp disc margins. |
| III / IV / VI | In addition to the observations below, dolls maneuver and cold water calorics were negative. |
| V | V1-V3 equal and symmetric to pinprick and temperature, sensation in mouth/oropharynx intact to pinprick, motor strong. |
| VII | Moderate to severe facial weakness on lip closure and eye closure bilaterally, labial weakness gives rise to slurred speech. |
| VIII | Hearing intact bilaterally. |
| IX / X | Palate and uvula elevates symmetrically, gag depressed bilaterally, gutteral sounds are weak. |
| XI | Sternocleidomastoid mildly weak bilaterally, trapezius strong bilaterally. |
| XII | Tongue midline, no atrophy, no fasciculations, strong. |
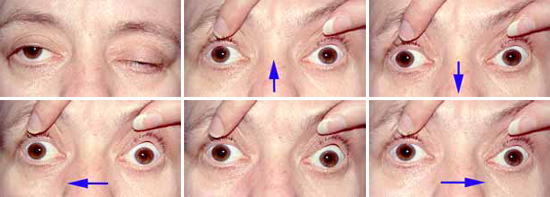
The patient is asked to look in the various positions of gaze, as indicated by the arrows.
Motor: Neck flexion 4/5, Neck extension 5/5, all other muscle groups 5/5. No atrophy, no fasciculations, and normal tone.
Reflexes: Absent throughout, Babinski and Hoffman not present.
Sensation: Intact to pinprick, temperature, vibration, proprioception.
Cerebellar: With one eye closed, patient had mild difficulty with finger to nose. Heel to shin was normal as well as rapid alternating movements.
Gait: Patient took several steps with assistance and felt unsteady and dizzy.
Email comments: