During an open approach or Ivor Lewis esophagectomy, a single incision is made in the abdomen. During a minimally invasive esophagectomy, typically six small incisions are made. The abdomen is filled with carbon dioxide to provide the surgeon with space to work.
We begin by exploring the abdomen to determine whether the cancer has spread to areas that aren’t removed during an esophagectomy. If it has spread to these areas, we stop the operation because these patients do not benefit from an esophagectomy.
Next, we separate the stomach, the lower esophagus and lymph nodes from the surrounding structures. We preserve one very important stomach artery in the process.

Creating Your New Esophagus
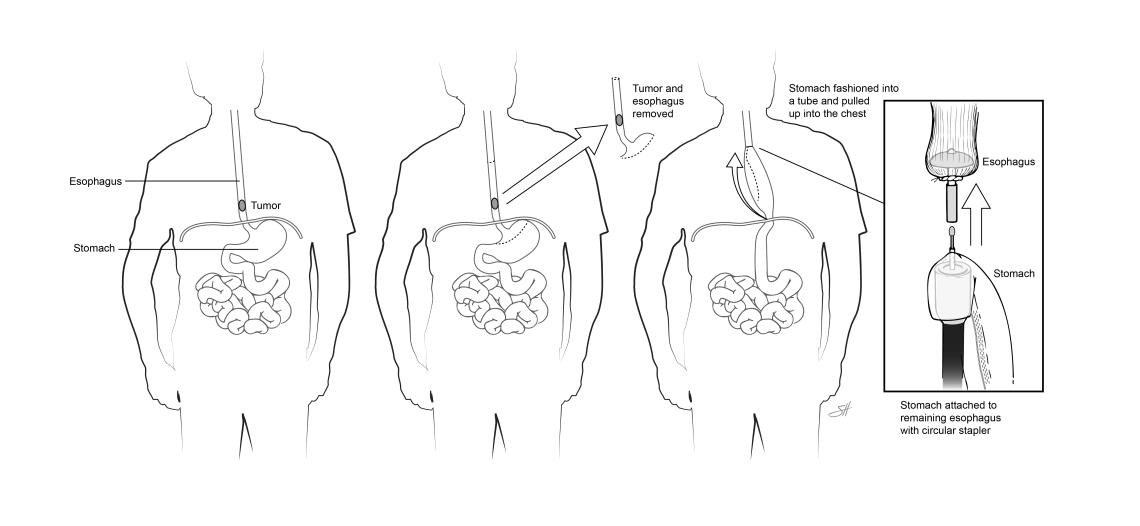
We then fashion a new esophagus out of your stomach. We use special staplers that both seal and cut tissue.
Unlike the esophagus that you were born with, your new esophagus (made out of your stomach) relies on gravity to drain its content into your abdomen. Anything that blocks the way between the stomach and the intestine can therefore adversely affect this drainage. This can lead to difficulty swallowing, bloating and aspiration.
There is a muscular structure between your stomach and the first portion of your intestine, which is called the pylorus. We will intentionally cut the pylorus (called a pyloromyotomy or pyloroplasty) to help the stomach empty its content better into the intestine.
We may prepare a portion of your omentum (a fatty apron of tissue in your abdomen) to wrap around the connection between your esophagus and stomach.
Finally, we place a temporary feeding tube (jejunostomy tube), if you don’t already have one. Nutrition is an important component of healing. Even though you will likely be taking in small amounts of liquids about a week after surgery, you won’t be able to eat enough protein by yourself for several weeks. The feeding tube is temporary and will be removed in the doctor's office when you no longer need it.
Your abdominal incisions are closed.
Next, we turn you on your side (right side facing up). Your right lung is collapsed during the procedure to allow us to get to your esophagus.
- Generally, we make five small incisions and one additional four-inch incision on your side.
- We free the esophagus and the lymph nodes from the opening in the diaphragm to the upper part of your chest, just below your neck.
- We cut the esophagus one-third of the way from the neck to the stomach and remove it.
- We then reconnect your esophagus to your new 'esophagus’ (your stomach).
- A chest tube is placed to help your lung re-expand and collect the normal amount of fluid that builds up after chest surgery. This tube is usually removed after two to three days.
- A smaller drain is placed behind the anastomosis (the connection between your stomach and esophagus) to collect fluid, in case a leak develops at this location.
- We check for leaks by looking at the color of the drainage and by obtaining a barium swallow after surgery. Small leaks will often heal with endoscopic management, as long as it is well-drained.
- The drain is left, in case you need it. If you don’t, we will back it out before you leave the hospital and remove it in the office at your first postoperative visit.
- A tube is placed down your nose and into the new esophagus to keep the pressure on the connection point low. This tube is usually removed after two days.