PLAIN RADIOGRAPHIC DIAGNOSIS OF CONGENITAL HEART DISEASE |
Contents | Previous Condition | Next Condition
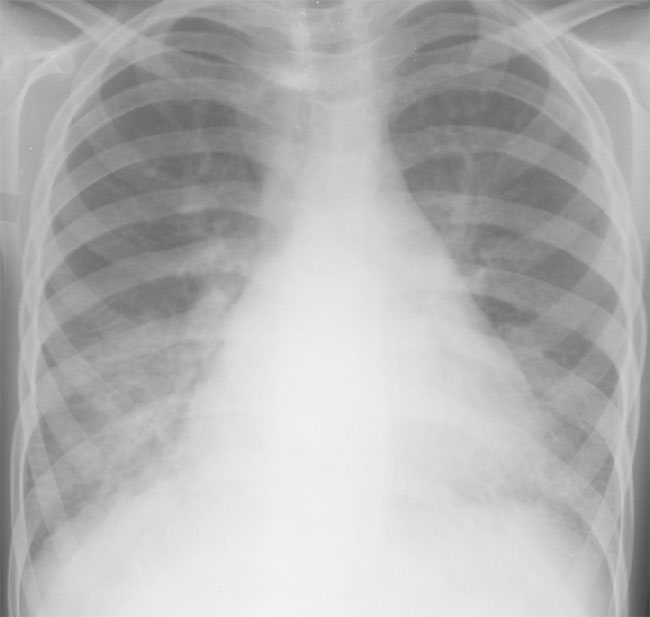
A. PA chest radiograph demonstrates moderate cardiac enlargement. The left atrium is extensively dilated and there are changes in each lower lobe secondary to longstanding passive venous congestion. There is fluid within the right horizontal fissure and mutiple bilateral septal lines (Kerley B) representing lymphatic engorgement in the costophrenic angles.
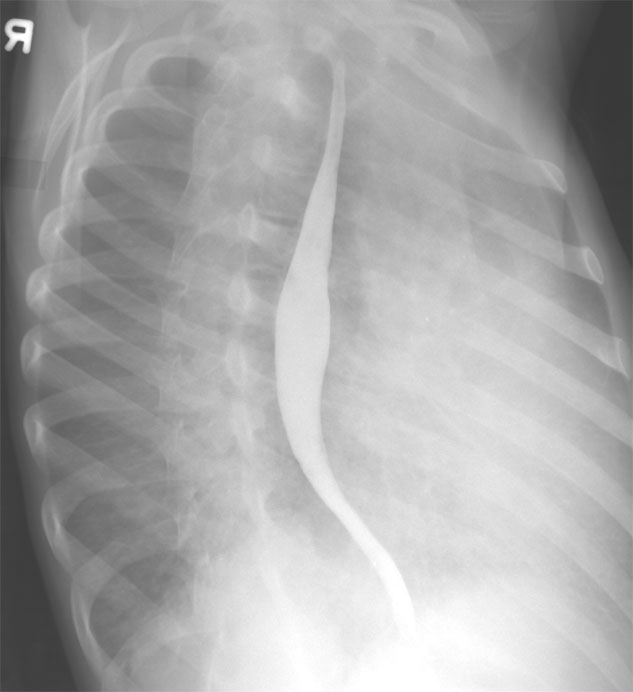
B. Right anterior oblique view confirms extensive left atrial dilation.
Mitral valve stenosis (MS) may be congenital or acquired, the latter being far more common in developing countries because of the prevalence of rheumatic fever. Congenital MS accounts for 0.5% of congenital heart disease. This may be isolated or associated with multiple left heart obstructive lesions (Shone’ syndrome).
Classification: There are five types of mitral stenosis; supravalvular, often secondary to a membrane, hypoplastic mitral valve annulus, parachute mitral valve, double-orifice mitral valve and hypoplastic left heart syndrome.
Physical findings: This is dependent upon severity and co-existent lesions.
The facies may have a reddish hue over the cheeks, so called "mitral facies".
The apex beat is tapping in nature. The first heart sound is soft with occasionally an opening snap following the second heart sound. There is a low frequency mid to late diastolic murmur loudest at the apex, which is accentuated on expiration. The presence of mitral regurgitation should always be sought. Elevated pulmonary pressures may be indicated by a pulmonary regurgitation murmur (Graham Steele murmur after the famous Manchester physician who described this in association with rheumatic MS).
In older patients the development of atrial fibrillation often accompanies the onset of pulmonary hypertension.
CXR: Moderate to severe stenosis is manifested by mild cardiomegaly with pulmonary venous congestion and left atrial enlargement. LAE has four characterisitc features, double atrial shadow, straight left heart upper border, an elevated left mainstem bronchus, and posterior displacement of the cardiac silhouette.
ECG: Left atrial enlargement, increased right ventricular forces, and a rightward axis.
ECHO: Careful analysis of the mitral valve structure, including estimation of the pressure half time and transmitral gradient using pulsed wave doppler.
Associations: Lutembacher described mitral stenosis in which there was relief of left atrial hypertension via an atrial septal defect masking the presence of MS.
Management: All patients require catheterization to accurately estimate transmitral gradient (simultaneous left atrial and left ventricular pressure readings), pulmonary artery pressure and resistance, and to calculate mitral valve annulus diameter (Gorlin formula).
Management: Medical therapy including digoxin, diuretics and anticoagulation may benefit in mild to moderate stenosis. Severe MS with elevated pulmonary artery pressures requires either valvuloplasty (e.g. divison of a parachute mitral valve) or valve replacement, which can be a significant problem in small children or children with hypoplastic valve annulus. Occasionally it may be necessary to implant a valve larger than the annulus in the supravalvular region. Balloon atrial septostomy may provide temporary relief in left atrial hypertension in chidren with significant MS.