PLAIN RADIOGRAPHIC DIAGNOSIS OF CONGENITAL HEART DISEASE |
Contents | Previous Condition | Next Condition
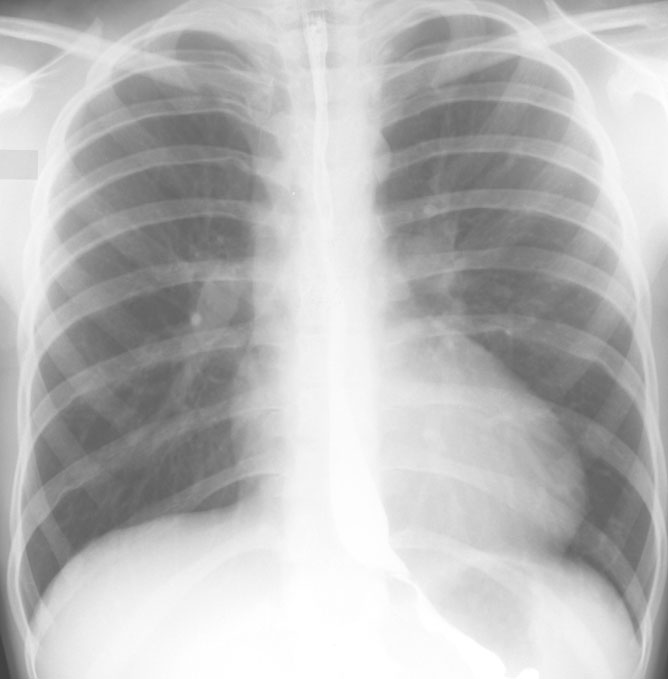
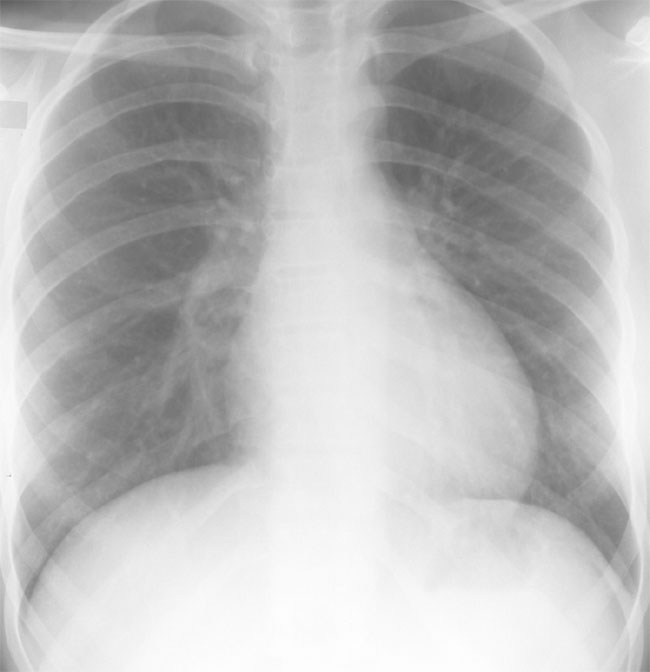
A. Chest radiograph demonstrates rib notching (ribs 3-8 bilaterally). There is a figure-three sign in the left upper mediastinum secondary to hypoplasia of the aortic arch with poststenotic dilation of the aorta infra-coarctation.
A. PA chest radiograph demonstrates rib notching/erosion of ribs 5-8 bilaterally (secondary to intercostal collateral development). There is cardiomegaly, figure-three sign in the left upper mediastinum and post-stenotic dilation of the descending aorta.

B. Left anterior oblique view shows slight anterior displacement of the esophagus by the dilated aorta below the coarctation.

A. PA chest radiograph shows bilateral rib notching (rib 5-8) with figure-3 sign and significant post-stenotic dilation of the descending aorta.
Coarctation in the adult is characterized by a short segment abrupt obstruction in the postductal region secondary to localized thickening of the aortic media. This typically occurs just distal to the ductus or ligamentum arteriosum. Infantile coarctation or preductal coarctation is characterized by a diffuse narrowing or hypoplasia of the aorta also in the presence of a discrete area of constriction in the aorta just beyond the origin of the left subclavian artery but proximal to the ductus arteriosus, hence distal blood supply is fulfilled via the ductus. Typical coarctation are those cases in which there is diffuse hypoplasia of the transverse arch in association with a discrete isthmic narrowing.
Incidence: Coarctation accounts for between 5-8% of all congenital heart defects. The male:female ratio is between 2-3:1 with an increased predisposition in girls with Turner’s syndrome (15-20%).
Associations: (1) Bicuspid aortic valve occurs in up to 85% of cases. (2) Ventricular septal defect (all types). (3) Mitral valve lesions including hypoplastic mitral valve, parachute mitral valve, and abnormal papillary muscles. (4) Shone’s syndrome (multiple left sided obstructions; supravalvular mitral ring, mitral valve stenosis, subaortic membrane/stenosis, aortic valve stenosis, coarctation). (5) Cyanotic congenital lesions including truncus arteriosus and transposition of the great arteries, especially with a subpulmonic VSD and overriding pulmonary artery (Taussig-Bing).
Physical findings: In later life characteristic features are upper limb hypertension with reduced or absent femoral impulses. Hypertension may not directly reflect the severity of the obstruction. If there is a higher left upper limb blood pressure relative to right, one should consider the possibility of an abberant right subclavian artery. The upper torso may be well developed relative to the lower torso. In infants there is less tendency to severe hypertension and the development of collaterals. There may be a thrill in the suprasternal notch. An ejection systolic murmur may be heard in the left upper sternal region, with an ejection click if there is an associated bicuspid aortic valve. The back should be palpated for the presence of collaterals and ausculted for continuous murmurs. Fundoscopic exam in older patients may yield evidence of hypertensive changes.
ECG: Often normal in early stages progressing to left ventricular hypertrophy. 50% of older patients may develop RBBB.
CXR: Characteristic features include post-stenotic dilation of the descending aorta, "figure 3" sign, and the development of rib notching secondary to dilated intercostal collateral vessels. This is reported in 70% patients between 6-41 years. It is extremely rare in infancy. Unilateral notching should alert one to the presence of ipsilateral anomalous subclavian artery arising below the coarctation (low pressure system, hence no collaterals).