PLAIN RADIOGRAPHIC DIAGNOSIS OF CONGENITAL HEART DISEASE |
Contents | Previous Condition | Next Condition
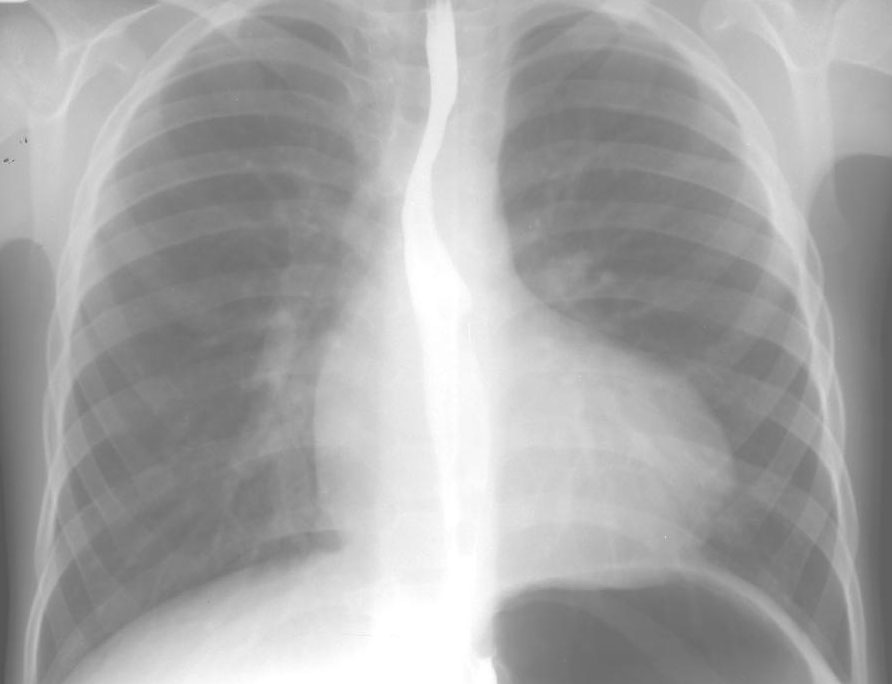
A. PA chest radiograph shows normal heart size which is "boot-shaped" (from coeur-en-sabot, literally translated boot shaped). There are diminished pulmonary vascular markings and a prominent left sided aortic arch (indentation in left of trachea).
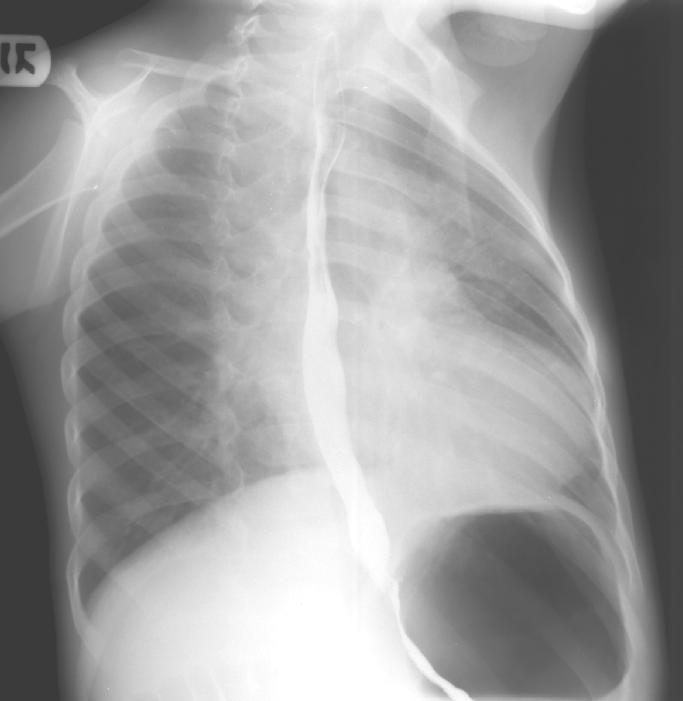
B. Right anterior oblique views shows upturned apex and decreased pulmonary vascular markings.
A. PA chest radiograph of a nine month old infant demonstrating normal cardiothoracic ratio with a boot-shaped heart, with decreased pulmonary vascular markings and a right aortic arch, which is present is 25% of children with tetralogy.

Tetralogy of Fallot, although previously described was detailed by Fallot in 1888 as part of a group of lesions he termed "maladie bleue". Tetralogy sequence consists of a ventricular septal defect (usually conoventricular), overriding of the aorta, pulmonary stenosis and right ventricular hypertrophy. The presence of "anterocephalad" deviation of the outlet ventricular septum defines this entity and gives rise to infundibular pulmonary stenosis as well as overriding of the aorta. Pentalogy of Fallot is tetralogy with co-existent atrial septal defect (as high as 82%). Other associated anomalies include the left anterior descending coronary artery running anterior to the right ventricular outflow tract, atrioventricular septal defect, left SVC to coronary sinus, aortopulmonary collaterals, supravalvular mitral stenosis, subaortic stenosis, hypoplasia or absence of a pulmonary artery and a right sided aortic arch. The presence of a right aortic arch is of practical importance to the surgeon as this determines the side of thoracotomy when performing a shunt procedure. A standard modified Blalock-Taussig shunt is performed on the contralateral side to the arch while a classic BT shunt (direct anastomosis of the subclavian artery to the pulmonary artery) is performed on the ipsilateral arch side.
Note: Tetralogy of Fallot may have a normal radiographic appearance particularly in "pink Tets" who have adequate pulmonary circulation either because of minimal right ventricular outflow tract obstruction or because of co-existent aorto-pulmonary collaterals. Indeed some patients may have evidence of clinical overcirculation secondary to excessive aorto-pulmonary collateral blood flow, manifested by high saturations and increased pulmonary markings on chest film. Individual cardiovascular lesions may represent heterogenous physiological entities and individual attention to clinical and radiographic features is vital to appropriate management. For example to shunt an infant with tetralogy with increased pulmonary blood flow would be catastrophic. Hence patients need to be assessed physiologically rather than as disease categories.