PLAIN RADIOGRAPHIC DIAGNOSIS OF CONGENITAL HEART DISEASE |
Contents | Previous Condition | Next Condition
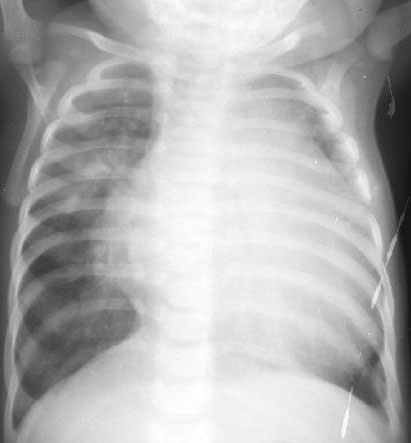
A. PA radiograph demonstrates only eleven sets of ribs. There is marked cardiomegaly with the left apex extending to the lateral chest wall. The pulmonary vascular markings are bilaterally increased and again air trapping can be appreciated in the right middle and left lower lung segments.
A. PA radiograph demonstrates cardiomegaly, increased pulmonary vascular markings. The finding of eleven pairs of ribs makes this diagnosis evident. The thymus gland is also appreciable.

These lesions are known by a number of terms including endocardial cushion defect, atrioventricular canal defect, canalis atrioventricularis communis, persistent atrioventricular ostium and the preferable term atrioventricular septal defect. These lesions involve a defect within the atrial and ventricular septum including involvement of one or both atrioventricular valves.
Classification:
The majority of patients have an abnormality of either or both mitral and tricuspid valves. The anterior or aortic leaflet of the mitral leaflet is abnormal in most patients. A cleft or gap is often present in the anterior and posterior leaflet of the mitral valve. Often the anterior and posterior leaflet of the tricuspid valve additionally has a cleft. The ventricular inlet septum is concave towards the atrium, with a resultant reduction in the ratio of the inlet to outlet distance of the ventricle. The left ventricular outflow is sprung anteriorly resulting in a characteristic elongated gooseneck appearance on AP cineangiograms. In PAVSD there are two atrioventricular valves while in CAVSD there is usually a common atrioventricular valve, which is composed of 5 leaflets. Two leaflets straddle the interventricular septum and are tethered by chordae in both ventricles; the anterior (or superior) and posterior (inferior) bridging leaflets. Two leaflets are located within the right ventricle and correspond to the anterior and posterior leaflets of the tricuspid valve. One leaflet is entirely within the left ventricle and is called the left lateral (mural) leaflet.
In 1966 Rastelli further classified CAVSDs on the basis of configuration of the superior bridging leaflet; superior bridging leaflet attached to the septum by chordae tendinae (Rastelli type A), superior brdging leaflet attached to the ventricular septum on the right side (Rastelli type B) and the superior bridging leaflet extending to the anterior papillary muscle within the right ventricle or "free-floating" (Rastelli type C).
Associated lesions: These include tetralogy of Fallot, ventricular dominance or hypoplasia (unbalanced AVSD), total or partial anomalous pulmonary venous drainage, interrupted IVC with azygos continuation, left superior vena cava to coronary sinus, left or right atrial isomerism, patent ductus arteriosus, and coarctation of the aorta.
Electrocardiogram: The most characteristic ECG finding is that of superior axis thought to be secondary to abnormally displaced conduction tissue with an associated abnormal cardiac activation sequence.
Prognosis: Patients with the best prognosis include patients with Down syndrome and Rastelli type C anatomy, with minimal atrioventricular valve regurgitation post-op in those patients.